Abstract
Lingual thyroid is a rare developmental anomaly caused due to the aberrant embryogenesis during descent of the thyroid gland from the foramen cecum to its pre-laryngeal site. Foreign body sensation in throat, dysphagia, dysphonia, pain and bleeding are the common presenting symptoms of this condition. Treatment includes the use of exogenous thyroid hormone to correct the hypothyroidism and to induce the shrinkage of the gland. Other treatment options include surgery and radiotherapy when symptoms of obstruction, bleeding and malignant transformation are present. Presented here is the case of a 39-year-old male presenting with foreign body sensation in throat of 1 week’s duration. The patient was diagnosed with lingual thyroid. Treatment with 50 µg/day of L-thyroxine was advised and surgery was deferred as the patient was asymptomatic.
Keywords: Lingual thyroid, ectopic thyroid, technetium-99m thyroid scan, L-thyroxine
Introduction
Lingual thyroid is a rare developmental anomaly caused due to the aberrant embryogenesis during descent of the thyroid gland to the neck. The first case of lingual thyroid was reported in 1869 by Hickman. Most frequent ectopic location (about 90%) of the thyroid gland is in the base of the tongue. Other sites include sublingual, thyroglossal and laryngotracheal, mediastinal and esophageal. Prevalence rate ranges from 1 in 1,00,000 to 1 in 3,00,000 population; 0.3% of cases will present in hypothyroid state. Diagnosis is mainly by clinical suspicion and confirmation by imaging.
Case Report
A 39-year-old male presented with foreign body sensation in throat of 1 week’s duration. There was no history of dysphagia, nocturnal dyspnea and sleep apnea/dysphonia. There were no signs of thyroid dysfunction. On intraoral examination, a globular lesion popped up near the mid-line of base of tongue on gagging (Fig. 1).
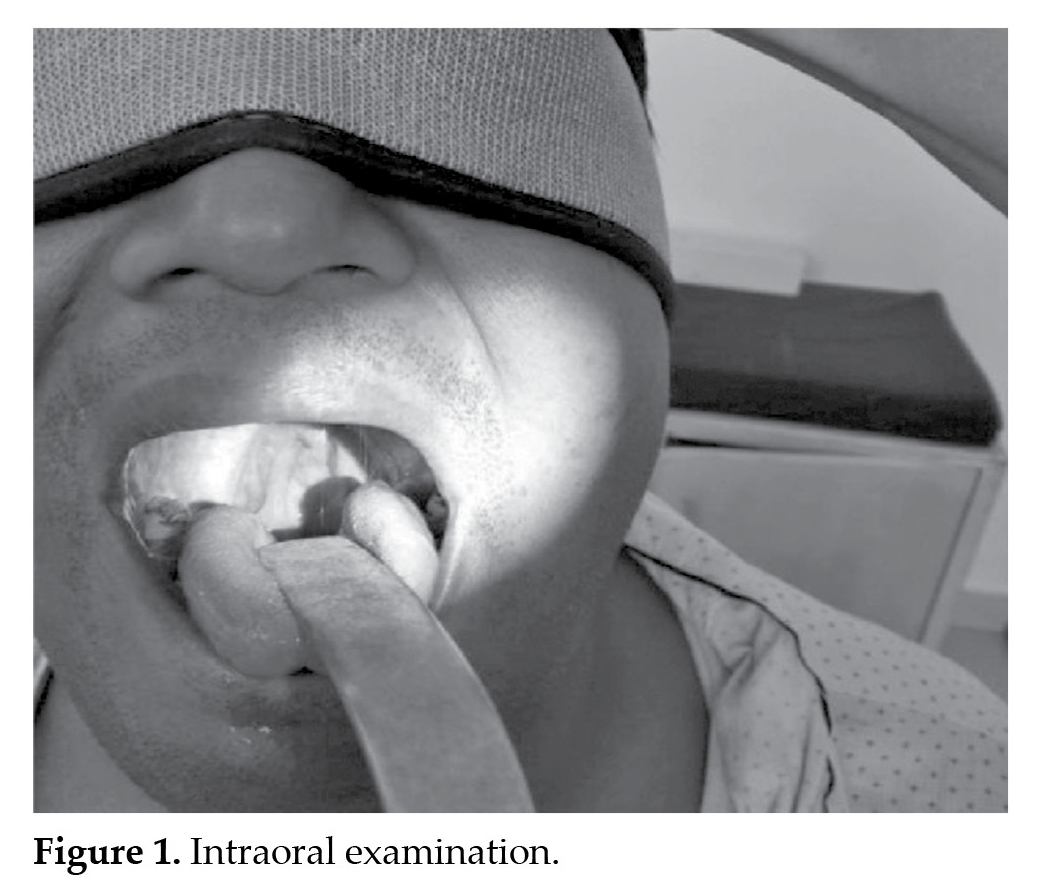
On videolaryngoscopy examination, a globular swelling measuring about 2.5 cm in diameter, smooth surfaced, extending from dorsal surface of base of tongue to lingual surface of epiglottis was noted. On palpation, the swelling was hard in consistency without any pain or discomfort. No bleeding points were seen. Ear, nose and neck examination was normal. Provisional diagnosis of lingual thyroid was made based on its location and appearance. The patient was advised for following investigations:
- Thyroid function test results showed the following parameters:
- Triiodothyronine (T3) - 1.22 ng/mL, thyroxine (T4) - 6.24 ng/mL and thyroid-stimulating hormone (TSH) - 14.29 mIU/mL
- T3 and T4 were measured by competitive electrochemiluminescent immunoassay
- TSH by sandwich electrochemiluminescent immunoassay.
- Ultrasonography of neck showed absent thyroid gland in thyroid fossa. Heterogeneous echo pattern solid lesion in the base of the tongue on the right side suggested lingual thyroid.
- Radionuclide thyroid scan and uptake study using 3 mCi of technetium-99m pertechnetate was done, which revealed abnormal radiotracer concentration in the base of tongue consistent with ectopic thyroid tissue. Thyroid gland was not visualized in its normal position. Thus, it indicated that this lingual thyroid is the only functioning thyroid gland.
The patient was advised 50 µg/day of L-thyroxine and surgery was deferred as the patient was asymptomatic.
Discussion
Lingual thyroid is the presence of ectopic thyroid tissue anywhere between circumvallate papillae of the tongue to epiglottis along the primitive thyroglossal duct. This is due to the embryonic failure of descent of normal thyroid tissue from foramen cecum area of base of tongue to the lower part of the neck in front of the thyroid cartilage. It has been hypothesized that the cause for the arrest in descent of thyroid anlage is due to the maternal antibodies against thyroid antigen.
The incidence of lingual thyroid is reported as 1 in 1,00,000. It is seven times higher in females when compared to males. About 33-62% of all patients have hypothyroidism with elevated levels of TSH.
Foreign body sensation in throat, dysphagia, dysphonia, pain and bleeding are the common presenting symptoms of this condition.
Investigation for lingual thyroid includes serum thyroid profile, radionuclide technetium-99m and iodine-131 thyroid scans. Other investigations include computed tomography (CT) and magnetic resonance imaging (MRI) of the neck with contrast, which helps in planning treatment. In our case, same radionuclide technetium-99m scan was done and abnormal radiotracer concentration in the base of the tongue was noted, consistent with ectopic thyroid tissue. Thyroid gland was not visualized in its normal position.
The treatment options that are available for lingual thyroid include surgery, radioiodine ablation and chemotherapy. The choice of treatment depends on symptoms such as dysphagia, sleep apnea, bleeding from the lesion, location and extent of the lesion.
Treatment of an asymptomatic patient in euthyroid state is regular follow-up. In hypothyroid patients, L-thyroxine is supplemented for suppressing the TSH levels as well as to reduce the size of the lesion. Indications for surgery include severe obstructive symptoms and complications such as bleeding, cystic degeneration or malignancy. Surgical excision may be considered after confirmation of adequate thyroid tissue in the neck by radioisotope scan. Surgical excision can be done either transorally or externally through a transhyoidal pharyngotomy. In patients lacking thyroid tissue in the neck, the lingual thyroid can be excised and implanted in the muscles of the neck.
In the present case, the patient was kept on hormone replacement therapy with L-thyroxine and was followed-up regularly every 3 months. Surgical excision was not considered in the present case as it was the only functioning thyroid gland. However, surgical excision can be considered in future, if malignant transformation occurs.
Conclusion
When a mass is observed in the base of tongue, ectopic lingual thyroid must be kept in mind for differential diagnosis. The diagnosis can be confirmed using ultrasonography, radionuclide thyroid scan, CT and MRI scans. Treatment option is based on symptomatology.
Suggested Reading
- Léger J, Marinovic D, Garel C, Bonaïti-Pellié C, Polak M, Czernichow P. Thyroid developmental anomalies in first degree relatives of children with congenital hypothyroidism. J Clin Endocrinol Metab. 2002;87(2):575-80.
- Hickman W. Congenital tumor of the base of the tongue, pressing down the epiglottis on the larynx and causing death by suffocation sixteen hours after birth. Trans Pathol Soc Lond. 1869;20:160-1.
- Abdallah-Matta MP, Dubarry PH, Pessey JJ, Caron P. Lingual thyroid and hyperthyroidism: a new case and review of the literature. J Endocrinol Invest. 2002;25(3):
264-7.
- Noyek AM, Friedberg J. Thyroglossal duct and ectopic thyroid disorders. Otolaryngol Clin North Am. 1981;14(1):187-201.
- Batsakis JG, El-Naggar AK, Luna MA. Thyroid gland ectopias. Ann Otol Rhinol Laryngol. 1996;105(12):996-1000.
- van der Gaag RD, Drexhage HA, Dussault JH. Role of maternal immunoglobulins blocking TSH-induced thyroid growth in sporadic forms of congenital hypothyroidism. Lancet. 1985;1(8423):246-50.
- Williams JD, Sclafani AP, Slupchinskij O, Douge C. Evaluation and management of the lingual thyroid gland. Ann Otol Rhinol Laryngol. 1996;105(4):312-6.
- Aktolun C, Demir H, Berk F, Metin Kir K. Diagnosis of complete ectopic lingual thyroid with Tc-99m pertechnetate scintigraphy. Clin Nucl Med. 2001;26(11):933-5.
- Kansal P, Sakati N, Rifai A, Woodhouse N. Lingual thyroid. Diagnosis and treatment. Arch Intern Med. 1987;147(11):2046-8.
- Toso A, Colombani F, Averono G, Aluffi P, Pia F. Lingual thyroid causing dysphagia and dyspnoea. Case reports and review of the literature. Acta Otorhinolaryngol Ital. 2009;29(4):213-7.
- Jones P. Autotransplantation in lingual ectopia of the thyroid gland. Review of the literature and report on a successful case. Arch Dis Child. 1961;36:164-70.
- Hari CK, Kumar M, Abo-Khatwa MM, Adams-Williams J, Zeitoun H. Follicular variant of papillary carcinoma arising from lingual thyroid. Ear Nose Throat J. 2009;88(6):E7.